OPEN ACCESS | Volume - Issue -
ISSN No: | Journal DOI:


Ashish K Mohapatra, MD, Cyril James, MD, FESC
Senior Consultant Interventional and Structural Cardiology Heart Failure Specialist Germany.
*Corresponding Author: Ashish K. Mohapatra, Senior Consultant Interventional and Structural Cardiology Heart Failure Specialist Germany.
Received date: July 14, 2023
Accepted date: July 19, 2023
published date: July 21, 2023
Citation: Ashish K. Mohapatra, James C. (2023) “Asymptomatic Severe Aortic Stenosis. A Journey of Patience or Proactivity? Analyzing Watchful Waiting and early intervention Strategy.” J Clinical Cardiology Interventions, 3(1); DOI: http;//doi.org/10.2023/07.1035.
Copyright: © 2023 Ashish K. Mohapatra. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background
According to ACC/AHA 2020 Guidelines, the asymptomatic severe aortic stenosis belongs to Stage C as per the staging classification of severe AS. There is a Class 1B recommendation for TAVI in Stage C2 in the case of a < 80 years old patient with a life expectancy of <10 years without contraindication for transfemoral TAVI. In ESC/ EACTS 2021 Guidelines, there is a Class 2A recommendation for intervention for asymptomatic severe AS. However, the decision-making for early TAVI in case of asymptomatic severe aortic stenosis still needs to be determined.
Methods
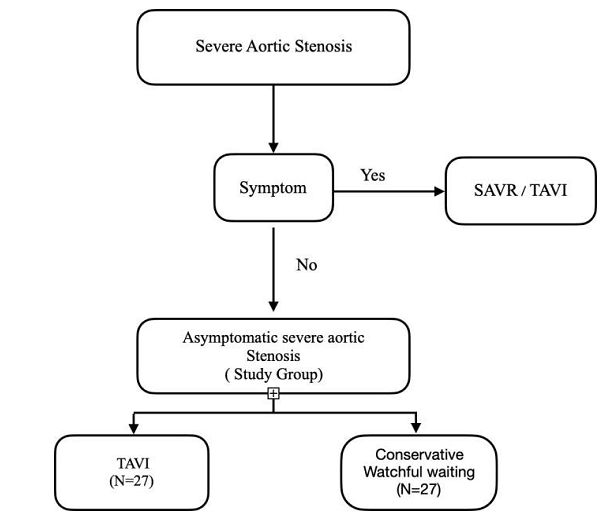
This prospective Study was initiated in October 2021, was conducted for 18 months, and was completed in March 2023. This study is a prospective multicenter study of asymptomatic severe aortic stenosis, candidates for Conservative treatment, and Transcatheter aortic valve implantation(TAVI). The patients satisfying the inclusion criteria without exclusion criteria were randomized 1:1 to early TAVI or conventional treatment.
Results
The age group of the mean(years)+/- 2SD(78+/-7.8) in the TAVI Group and (77+/- 7.7) in the Watchful waiting group. The Aortic Valve area of the TAVI Group (mean) was 0.81cm2(062-0.95), and the watchful waiting group was 0,82cm2 (0.64-0.94)— follow-ups in every 3 months with clinical examination and echocardiography with LV-GLS, LVMI, and LAVI measurements. In 12 monthly follow-up periods, a LAVI regression of 15.48% was observed. Likewise, an LMVI Reduction of 11.83% was noted. Most importantly, LV-GLS improved by 22.79% in 12 months of the study period.
Conclusion
In conclusion, based on the findings of this investigation, transcatheter aortic valve implantation (TAVI) outperforms watchful waiting in patients with asymptomatic severe aortic stenosis (AS). TAVI significantly improves cardiac function parameters, reducing the risk of adverse events, including heart failure and major cardiovascular events, while improving the quality of life.
Introduction.
Background and Rationale
The significant narrowing of the aortic valve characterizes severe aortic stenosis. It may lead to chest pain, shortness of breath, fatigue, and fainting. However, in some cases, individuals with severe aortic stenosis may remain asymptomatic.
When managing asymptomatic severe aortic stenosis, there are two main approaches: watchful waiting and Early Intervention. The Intervention is of two types; one is surgical aortic valve replacement(SAVR), and the other one is minimally invasive transcatheter aortic valve implantation (TAVI).In this prospective study, we will discuss Watchful waiting and early TAVI.
Watchful Waiting: Watchful waiting involves regular monitoring of the patient's condition with serial echocardiograms and clinical assessments. This approach is typically considered for asymptomatic patients with minimal symptoms.
The rationale behind watchful waiting is that some individuals with severe aortic stenosis may remain asymptomatic for an extended period, and the risks associated with Intervention may outweigh the potential benefits in these cases.
Early Intervention (TAVI): Transcatheter aortic valve implantation (TAVI) is a less invasive percutaneous procedure; It involves inserting a prosthetic valve through a catheter, typically transfemoral or, in some particular cases, trans axillary or transaortic or transcranial or transapical. TAVI has been established as a viable alternative to surgery, particularly for high-risk or inoperable patients.
The rationale for early Intervention with TAVI in asymptomatic severe aortic stenosis is based on several factors. Firstly, evidence suggests that early Intervention may improve outcomes compared to delaying treatment until the onset of symptoms, and secondly, delaying Intervention until symptoms may be associated with a higher risk of complications, including sudden cardiac death. Lastly, TAVI has shown favorable outcomes in high-risk patients, making it a viable option for early Intervention in selected asymptomatic cases.
According to ACC/AHA 2020 Guidelines, the asymptomatic severe aortic stenosis belongs to Stage C as per the staging classification of severe AS.(1) Stage C is further classified into C1 And C2 depending on aortic valve morphology and left ventricular dysfunction as per ACC guidelines surgical AVR has a class 1B recommendation in case of Stage C2 and for Stage C1 with an indication for other cardiac surgery. (2,3,4). However, there is a Class 1B recommendation for TAVI in Stage C2 in the case of a < 80 years old patient with a life expectancy of <10 years without contraindication for transfemoral TAVI(5). Whereas in ESC/EACTS 2021 Guidelines, there is a Class 2A recommendation for intervention for asymptomatic severe AS. (6)
Two trials named AVATAR Trial (Aortic Valve Replacement vs. Conservative Treatment in Asymptomatic Severe Aortic Stenosis). and RECOVERY Trial (The Randomized Comparison of Early Surgery vs. Conventional Treatment in Very Severe Aortic Stenosis) compared early surgical AVR and watchful waiting and concluded that, early surgery results in improved survival and reduced hospitalization compared to conservative treatment. (7,8). At the same time, no randomized controlled trials have compared early TAVI with a watchful waiting strategy in asymptomatic severe AS. It is worth mentioning here that there is one Trial comparing early TAVI with conservative management (EARLY TAVR.
Trial(NCT03042104))is in progress, two ongoing Trials for early SAVR in asymptomatic severe AS ( EVOLVED Trial (NCT03094143) and ESAY-AS Trial(NCT04204915) and one ongoing Trial comparing early intervention(SAVR/ TAVR) with conservative (DANAVR-NCT03972644). This prospective study sought to compare the clinical outcomes of early TAVI with those of conventional management in asymptomatic patients with severe AS.
Research Methodology
Research Objective
The primary objective of this prospective study is to compare the benefit of early Transcatheter Aortic Valve Implantation(TAVI) with those of a conservative treatment strategy with asymptomatic severe aortic stenosis.
Research Design
This study is a prospective multicenter study of asymptomatic severe aortic stenosis, candidates for Conservative treatment, and Transcatheter aortic valve implantation(TAVI). The patients satisfying the inclusion criteria without exclusion criteria were randomized 1:1 to early TAVI or conventional treatment.
Limitations of this Study
The final Study Patient number was reduced because of Noncompliance and withdrawal of Participation in this study. Finally, after one month of Study, the study population remained stable, with 25 Patients in each group. Because of financial constraints, the laboratory Test of NT Pro BNP was not considered one study parameter. As compliance for this study is relatively better in males than females in India, this short-term prospective study was conducted taking male patients.
Inclusion Criteria
Exclusion Criteria
|
|
||||||
|
0 Month |
3 Months |
6 Months |
9 Months |
12 Months |
15 Months |
18 Months |
Study parameters
Serial echocardiograms in stipulated study intervals measured these three Study parameters. The Patients were given a study Schedule for a physical presence at study intervals in their respective centers.
Transcatheter Aortic Valve Implantation (TAVI)
The Patients of the TAVI group underwent Transfemoral TAVI(TF-TAVI) only. This group of patients had undergone coronary angiograms before inclusion in this study, as Coronary artery Disease is one of the Exclusion criteria. All the Patients were followed after TAVI in 3 months, 6 months, 9 months, 12 months,15 months, and 18 months.
Conservative Watchful Waiting-
The patients assigned to the conservative treatment group were managed with medicines per the current guidelines. The Patients were informed to communicate with their respective centers if they develop symptoms such as Angina, dyspnoea, or Syncope for further evaluation and early surgical Aortic Valve replacement or Transcatheter Aortic valve implantation. This Patient group was followed at the stipulated intervals of 3 months, 3 months, 6 months, 9 months, 12 months, 15 months, and 18 months without fail.
Results
|
Study |
TAVI Group |
Watchful Waiting Group |
|
Age (Years)(mean +/- 2 SD) |
78 +/- 7.8 |
77 +/- 7.72 |
|
AorticValve Area(cm2) (Mean) |
0.81(0.62-0.95) |
0.82(0.64-0.94) |
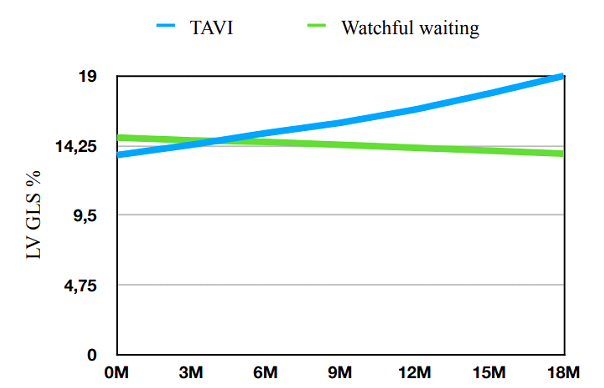
Left ventricular Global longitudinal strain(LV-GLS)
According to the meta-analysis, the Left ventricular global longitudinal strain (LV- GLS) < -16% signifies impaired myocardial dysfunction even if in average Left ventricle ejection Fraction. (9) Considering the multicenter study using different Echocardiography machines, and different echocardiographers, we have taken <-16% as the cutoff value for LV GLS in this prospective study and evaluate the effect of both strategies on GLS.
|
0M |
3M |
6M |
9M |
12M |
15M |
18M |
|
|
TAVI(me an) |
-13.6 |
-14.3 |
-15.1 |
-15.8 |
-16.7 |
-17.8 |
-19 |
|
Watchful waiting (mean) |
-14.8 |
-14.6 |
-14.5 |
-14.3 |
-14.1 |
-13.9 |
-13.7 |
TAVI Watchful waiting
|
0M |
3M |
6M |
9M |
12M |
15M |
18M |
|
|
TAVI(me an) |
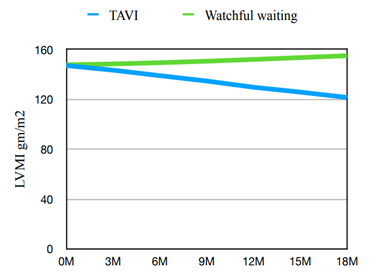
147.1 |
143.4 |
139.0 |
134.7 |
129.7 |
125.8 |
121.5 |
|
Watchful waiting (mean) |
147.7 |
148.4 |
149.4 |
150.6 |
152.0 |
153.5 |
155 |
* study conducted on male patients only.
TAVI Watchful waiting
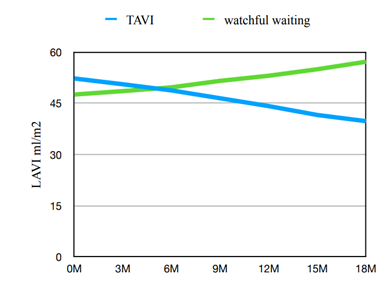
Left Atrial Volume Index(LAVI)
LAVI was an independent predictor of adverse events in patients with moderate or severe AS and preserved ejection fraction. Patients may improve risk stratification by including LAVI in the AS risk assessment. (13)
The size of the left atrium is smaller in the case of the South Asian population compared to its Western counterpart. (14) For this study, LAVI <30 ml/m2 is considered normal, and >30 ml/m2 I considered decreased.
|
0M |
3M |
6M |
9M |
12M |
15M |
18M |
|
|
TAVI(me an) |
52,3 |
50,6 |
48,8 |
46,5 |
44,2 |
41,6 |
39,8 |
|
Watchful waiting (mean) |
47,6 |
48,6 |
49,7 |
51,6 |
53,1 |
55 |
57,2 |
TAVI watchful waiting
Result of the Study.
Fifty-four patients with asymptomatic severe aortic stenosis were included in this prospective study, with a follow-up time of 18 months. Because of compliance problems, the number of participants was readjusted to 50. 50 % of patients underwent transcatheter aortic valve implantation(TAVI), and 50% experienced a watchful waiting strategy. The age group of the mean(years)+/- 2SD(78+/-7.8) in the TAVI Group and (77+/- 7.7) in the Watchful waiting group. The Aortic Valve area of the TAVI Group (mean) was 0.81cm2(062-0.95), and the watchful waiting group was 0,82cm2 (0.64-0.94). During this Study, in 3 months study intervals, all the patients of both groups were examined clinically and underwent echocardiography. In the follow-up measurements of LV-GLS, LVMI, and LAVI, it was noted that there is substantial improvement in each echocardiographic parameter after TAVI in the case of asymptomatic patients. (as shown in the graphs).In 12 monthly follow-up periods, a LAVI regression of 15.48% was observed. Likewise, an LMVI Reduction of 11.83% was noted. Most importantly, LVGLS improved by 22.79% in 12 months of the study period.
Discussion
This multicenter prospective study compared TAVI versus conservative treatment in individuals with asymptomatic severe aortic stenosis. The study found that patients with early percutaneous intervention (TAVI) had significantly better left ventricular and left atrial function over the follow-up period than those who received conservative therapy. Furthermore, early intervention was linked to enhanced quality of life in these individuals.
In an asymptomatic patient, the choice to undergo TAVI necessitates carefully evaluating the risks of aortic-valve replacement against the hazards of cautious waiting. In individuals with asymptomatic severe aortic stenosis, it appears safe to use an anticipatory waiting strategy and postpone intervention until symptoms occur.
(15) However, this conservative treatment approach has been linked to patient denial of symptoms, deterioration of cardiac functions, and increased intervention risk and complications while waiting for symptoms to develop. (16)This is quite evident from this prospective study as well.
Conclusion
In conclusion, based on the findings of this investigation, transcatheter aortic valve implantation (TAVI) outperforms watchful waiting in patients with asymptomatic severe aortic stenosis (AS). TAVI significantly improves cardiac function parameters, reducing the risk of adverse events, including heart failure and major cardiovascular events, while improving the quality of life.
Although procedural complications were observed with TAVI, they did not outweigh the significant benefits observed. Therefore, TAVI emerges as a favorable intervention for asymptomatic severe AS, providing patients with improved outcomes and potentially preventing the progression of cardiac dysfunctions. Further research and long-term follow-up studies are warranted to validate these findings and establish the long-term effectiveness and safety of TAVI in this specific patient population.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org